Nephrology
Why Are You Still Avoiding PD in Older Adults?
Interactive Case Study
This interactive case study was organised and funded by Vantive Global Medical Affairs Technical & medical writer support was provided by EMJ.
1/22
Disclosure These interactive case studies were developed with support from Professor Peter Rutherford, Global Head of Medical, Vantive LLC.
Disclaimer This is a hypothetical patient case and outcomes may not be reflective of clinical studies or real-life circumstances. This includes reference to agents that may be used off-label or for unlicensed indications. The mention of these agents and their uses is intended solely for educational purposes and should not be considered an endorsement or recommendation for their use outside approved indications. Please always consult guidelines and local prescribing information in your country of practice, as information may vary.
2/22
This is your first day in a new clinic and a patient is approaching the need for dialysis. Referral notes detail that she is at high risk of needing dialysis within the next few months.
In this interactive case study, you will: Identify the patient’s treatment needs with a clinical examination Evaluate the patient’s social factors that affect their decision-making on treatment Implement additional assessments to support the use of suitable treatments
Case Presentation: Female aged 78 years old
3/22
Age: 78 Sex: Female BMI: 24.1 BSA: 1.73 m2 (Du Bois)
Medical History:
Diagnoses:
Hypertensive Nephrosclerosis Hyperlipidaemia Hypertension Osteoarthritis PVD CAD Hyperkalaemia Peripheral oedema Albuminuria
BSA: body surface area; CAD: coronary artery disease; PVD: peripheral vascular disease.
Coronary artery disease:
Hyperlipidaemia
Hypertension
Hyperkalaemia
Oedema
Osteoarthritis
Peripheral Vascular Disease
Albuminuria
Hypertensive nephrosclerosis
4/22
Blood tests: GFR: 15 mL/min/1.73 m² BUN: 1.43 mmol/L (4 mg/dL) Glucose: 6.1 mmol/L (110 mg/dL) CO₂: 20 mmol/L (20 mEq/L) Ca: 1.85 mmol/L (7.4 mg/dL) Na: 145 mmol/L (145 mEq/L) K: 6.4 mmol/L (6.4 mEq/L) Chloride: 78 mmol/L (78 mEq/L) Hgb: 6.1 mmol/L (9.9 g/dL) Albumin: 37 g/L (3.7 g/dL) Phosphorus: 1.45 mmol/L (4.5 mg/dL) Bicarbonate: 20 mmol/L (20 mEq/L)
Medical Examination: Laboratory Results
BUN: blood urea nitrogen; CO2: carbon dioxide; Ca: calcium; Na: sodium; K: potassium; Hgb: hemoglobin; PCR: Protein-to-Creatinine ratio; GFR: glomerular filtration rate; uACR: urine-albumin-creatinine ratio.
Urine tests: PCR: 90.5 mg/mmol (800 mg/g) Protein: Present uACR: 80 mg/mmol (707 mg/g)
Is the patient at risk of Kidney Failure? Use the Kidney Failure Risk Equation to find out.
Calculating Kidney Failure Risk
THE PROJECTED RISK OF KIDNEY FAILURE
URINE
SEX
AGE
GLOMERULAR FILTRATION RATE
Click to reveal patient data:
uACR: Sex: Age: GFR:
Ca: calcium; GFR: glomerular filtration rate; uACR: urine-albumin-creatinine ratio.
5/22
Using the patient's Urine, Sex, Age, and GFR, the kidney failure risk equation1 provides the 2 and 5 year probability of treated kidney failure for a potential patient with CKD Stage 3 to 5. 1. Kidney Failure Risk Calculator. Available at: https://www.kidneyfailurerisk.com/. Last accessed: 27 March 2025.
For further information on calculating kidney function risk, use the Kidney Failure Risk Equation, see resources at the end of case study.
Reveal
80 F 78 15
For improved accuracy, additional parameters are included:
Albumin: Phosphorous: Bicarbonate: Ca:
37 1.45 20 1.85
Click to calculate the projected risk of kidney failure using patient parameters.
Calculate
The Kidney Risk Equation identifies the patient as requiring dialysis:
STAGE 4: Severe decrease in function Potential risk of progression to kidney failure requiring dialysis or transplant: AT 2 YEARS - 48.99% AT 5 YEARS - 88.84%
NO OR SLIGHT MILD MODERATE SEVERE APPROACHING FAILURE CKD Stages
>90 89–60 59–30 29–15 <15 Glomerular filteration rate
1 2 3 4 5
Is The Patient Suitable for Peritoneal Dialysis?
YES
NO
The patient is suitable for peritoneal dialysis. Let's explore this opportunity further
Correct, the patient is suitable for peritoneal dialysis. Continue to explore key outcomes and patient considerations
6/22
What outcomes associated with peritoneal dialysis do you expect for elderly patients?
1. Jiang C et al. Outcomes of peritoneal dialysis in elderly vs non-elderly patients: a systemic review and meta-analysis. PLOS ONE. 2022;17(2):e0263534.
A
B
C
D
F
E
An increase in the number of comorbidities Increase in functional decline Psychosocial issues with self-care Higher risk of complications associated with the use of peritoneal dialysis Decreased choice of peritoneal dialysis as a treatment modality None of the above
None of the above
Answer is F All elderly patients, not just those with kidney failure, have an increase in the number of comorbidities, functional decline, and psychosocial issues with self-care. The same percentage of elderly would choose peritoneal dialysis as a renal replacement therapy as compared to the general End Stage Kidney Disease (ESKD) population.1
7/22
Survival Difference of Elderly Patients on Dialysis
1. Segall et al. Dialysis modality choice in elderly patients with end-stage renal disease: a narrative review of the available evidence. Nephrol Dial Transplant. 2017;32(1):41-9
For elderly patients, survival duration between hemodialysis and peritoneal dialysis, even when statistically significant, is usually in the range of months, given the short survival on dialysis of these patients, in general.1 This aspect should be discussed with elderly patients starting on dialysis, during presentation and discussion of treatment options.
Deciding on treatment options, especially with elderly patients, should be a discussion that involves the patient’s quality of life, social factors, and wishes.
8/22
Medical Examination: Social Factors
Independence Peritoneal dialysis supports patient independence by enabling greater autonomy and flexibility at home.
The patient volunteers at a local church and would like to continue to contribute her time. She performs activities of daily living without assistance. The patient has mild cognitive impairment in that she is forgetful, but it currently does not interfere with her everyday life.
How might social factors inform dialysis suitability? Click to explore key themes:
1
Support system Home dialysis, including peritoneal dialysis, can provide a safe, viable option for elderly patients —particularly those without support systems or with physical or cognitive limitations.
The patient lives alone with support from her daughter and several church members. They transport her to doctor’s appointments, church, the pharmacy, and grocery store.
2
Physical Ability, Dexterity Home dialysis, particularly peritoneal dialysis, can be tailored to accommodate patients with varying levels of physical ability and dexterity.
The patient knits blankets for her family and the church. She moves slowly but has a steady gait.
3
4
Further assessments are scheduled in the clinic to assess dialysis options.
9/22
What would you assess?
ADL: activities of daily living Brown et al. International Society for Peritoneal Dialysis practice recommendations: prescribing high-quality goal-directed peritoneal dialysis. Perit Dial Int. 2020;40(3):244-53. Bonenkamp et al. Key elements in selection of pre-dialysis patients for home dialysis. Perit Dial Int. 2021;41(5):494-501.
Answer is E Functional, social and cognitive assessments facilitate shared decision making between the patient and health care practitioner and empower the patient to discuss and achieve their life goals whilst still receiving high-quality dialysis care.1 Many elderly patients are keen for an at-home therapy that has less intrusion on their daily life; home assessments facilitate the access of elderly patients to peritoneal dialysis where it is manageable and appropriate.2
Functional assessment (ADL) Social support assessment Home assessment Dementia assessment All of the above
All of the above
Submit
10/22
Assessing patient factors
Space Adequate room for supplies and equipment Free of distractions (privacy if possible) Stable temperature (no extremes) Safety Adequate lighting Electrical safety (outlets are in good condition) Ergonomics Minimise physical strain Machine and supplies are at appropriate height
Please note:
Cognitive assessment: Dementia Severity Rating Scale (DSRS) A functional assessment of a patient’s cognitive and daily living abilities regarding dementia. The scale assesses impairment across 12 domains including: memory, speech and language, recognition of family members, orientation to time and place, and decision-making. Patients are scored based on severity in each domain, with higher scores indicating greater impairment: Score of 0–6: No or minimal impairment Score of 7–17: Mild cognitive decline Score of 18–36: Moderate dementia Score of 37–54: Severe dementia
Social assessment: Multidimensional Scale of Perceived Social Support A self-reported assessment of perceived social support. The scale evaluates perceived support in three domains: Significant Other, Family, and Friends. Patients rate their agreement with 12 statements on a 7-point scale, from Very Strongly Disagree (1) to Very Strongly Agree (7). Scoring is based on the average ratings across different support sources as well as an overall total score: Score of 1–2.9: Low perceived support Score of 3–5: Moderate perceived support Score of 5.1–7: High perceived support
Functional assessment: KATZ Index of Independence in Activities of Daily Living (KATZ ADL) A functional assessment of a patient's ability to perform activity of daily living independently. The index ranks adequacy of performance in six functions: bathing, dressing, toileting, transferring, continence, and feeding. Patients are scored yes/no for independence of each function with a lower score indicating greater impairment: Score of 6: Full function Score of 4: Moderate impairment Score of 2: Severe functional impairment
Please note that these are example assessments from a US perspective, and other assessments are available. Refer to full versions via the resource section (also available at the end of the case study).
Home assessment: Does the patient have a safe place for doing an exchange?
Space Adequate room for supplies and equipment Free of distractions (privacy if possible) Stable temperature (no extremes) Saftey Adequate lighting Electrical safety (outlets are in good condition) Ergonomics Minimise physical strain Machine and supplies are at appropriate height
11/22
Kidney Failure Risk Equation: https://kidneyfailurerisk.com/ KATZ Index of Independence in Activities of Daily Living (KATZ ADL): https://hign.org/sites/default/files/2020-06/Try_This_General_Assessment_2.pdf Dementia Severity Rating Scale (DSRS): https://tmdf.org/wp-content/uploads/2020/07/Dementia-Severity-Rating-Scale.pdf Multidimensional Scale of Perceived Social Support: https://tmdf.org/wp-content/uploads/2020/07/Dementia-Severity-Rating-Scale.pdf
Assessment Results:
Click the to explore the results of the home visit.
Home assessment: Does the patient have a safe place for doing an exchange? Yes: The patient has adequate lighting at home and outlets are in good condition.
Home assessment: Does the patient have a safe place for doing an exchange? The patient has adequate room for supplies and equipment. The location of the machine minimises physical strain and supplies are at an appropriate height.
The patient’s assessment results: KATZ index of independence in ADLs: Moderate impairment Cognitive assessment: Mild impairment Social Support assessment: High perceived support
12/22
What are the five most important concerns this patient may have when making a decision?
Wong B et al. Selection of peritoneal dialysis among older eligible patients with end-stage renal disease. Nephrol Dial Transplant. 2017;32(2):384-92.
Maintaining a normal life Dietary changes Burden on others Transportation to and from the clinic Home environment separate from hospital Keeping a sense of purpose Night therapy and effect on sleep Dependence on others
G
H
Answer is A, C, E, G, and H Modality selection in elderly patients covers three main themes:1 Capability: Having a sound mind, physical strength and dexterity Motivation: Maintaining a normal life, burden or dependence on others, home environment separate from the hospital, night therapy, and effect on sleep Opportunity: Support from others, employment, and external influences
13/22
How Older Adults Make Decisions
1. Carstensen LL, Mikels, JA. At the intersection of emotion and cognition: aging and the positivity effect. Curr Dir Psychol Sci. 2005;14(3):117-21. 2. Mikels et al. Older adults place lower value on choice relative to young adults. J Gerontol B Psychol Sci Soc Sci. 2009;64(4):443-6.
Did you know that the way older adults make decisions differs substantially from the way younger adults do? Emotional functioning and regulation improve with age, so older adults are more likely to focus on and remember positive information.1 Older adults do not desire or value choice to the same extent that younger adults do.2
When encouraging older adults to make a complex decision, focus on their feelings as opposed to specific details and not only will they make better decisions, but they will also be more satisfied with their decision.
The number of options should be limited to allow a higher quality decision that they will be more satisfied with.
14/22
Quality of Life in Elderly patients
Brown EA et al. Broadening Options for Long-term Dialysis in the Elderly (BOLDE): differences in quality of life on peritoneal dialysis compared to haemodialysis for older patients. Nephrol Dial Transplant. 2010;25(11):3755-63 Sandrine G et al. Prognostic survival factors in elderly renal failure patients treated with peritoneal dialysis: a nine-year retrospective study. Perit Dial Int. 2010;30(2):218-26.
Percentage of patients choosing peritoneal dialysis worldwide:
Gao L et al. Outcomes of elderly peritoneal dialysis patients: 65-74 years old versus ≥ 75 years old. Ren Fail. 2023;45(2):2264977. Couchoud C. Associations between comorbidities, treatment choice and outcome in the elderly with end-stage renal disease, Nephrol Dial Transplant. 2007;22(11):3246-54 Yang, X et al. Clinical outcomes of elderly patients undergoing chronic peritoneal dialysis: experiences from one center and a review of the literature. Int Urol Nephrol 2007;39:1295-302 Kam-Tao Li P et al. Success of the peritoneal dialysis programme in Hong Kng, Nephrol Dial Transplant. 2008;23(5):1475-8 Li Y et al. Long-term survival of elderly peritoneal dialysis patients. Chinese Journal of Nephropathy. 2017;33(01):1-7.
France1,2
Canada1,3
China1,5
Hong Kong1,4
35% of patients over 85 years old chose peritoneal dialysis.1,2
41% of patients over 65 years old.1,3
42% of elderly patients.1,5
80% of patients approximately 62 years old.1,4
80
Individualised dialysis modalities to improve quality of life are important for older patients. Peritoneal dialysis is more suitable for elderly patients as it has less intrusion on their daily life.1 Consequently, a higher percentage of elderly patients chose peritoneal dialysis. Click here to see more: It is likely that the proportion of elderly patients undergoing peritoneal dialysis will increase in the future.2
15/22
%
35
41
42
What principles would you apply when providing modality education to this patient?
HCP: healthcare professional. Segall L. Dialysis modality choice in elderly patients with end-stage renal disease: a narrative review of the available evidence. NDT. 2017; 32(1):41-9.
Include family members in the process Re-assess well-being and satisfaction with choice should be regularly assessed Focus on their feelings Group choices into smaller chunks to decrease the number of options Consider the burden of all co-morbidities All of the above
Answer is F Dialysis modality choice should be patient-centred and tailored to individual needs, reflecting the well-informed preferences of the patient, unless contraindicated.1 Family involvement supports shared decision-making, while regular reassessment and attention to the patient’s feelings enhance adherence and quality of life. Simplifying choices into manageable chunks aids decision-making, especially for those with cognitive limitations. Considering co-morbidities ensures alignment with the patient’s physical and health needs, optimising outcomes.
16/22
Starting Peritoneal Dialysis
Reference
Now that your patient has selected their treatment of choice, steps must be taken to ensure they are ready to begin therapy.
Identifying the dialysis clinic and introducing the patient and caregiver to the clinicians.
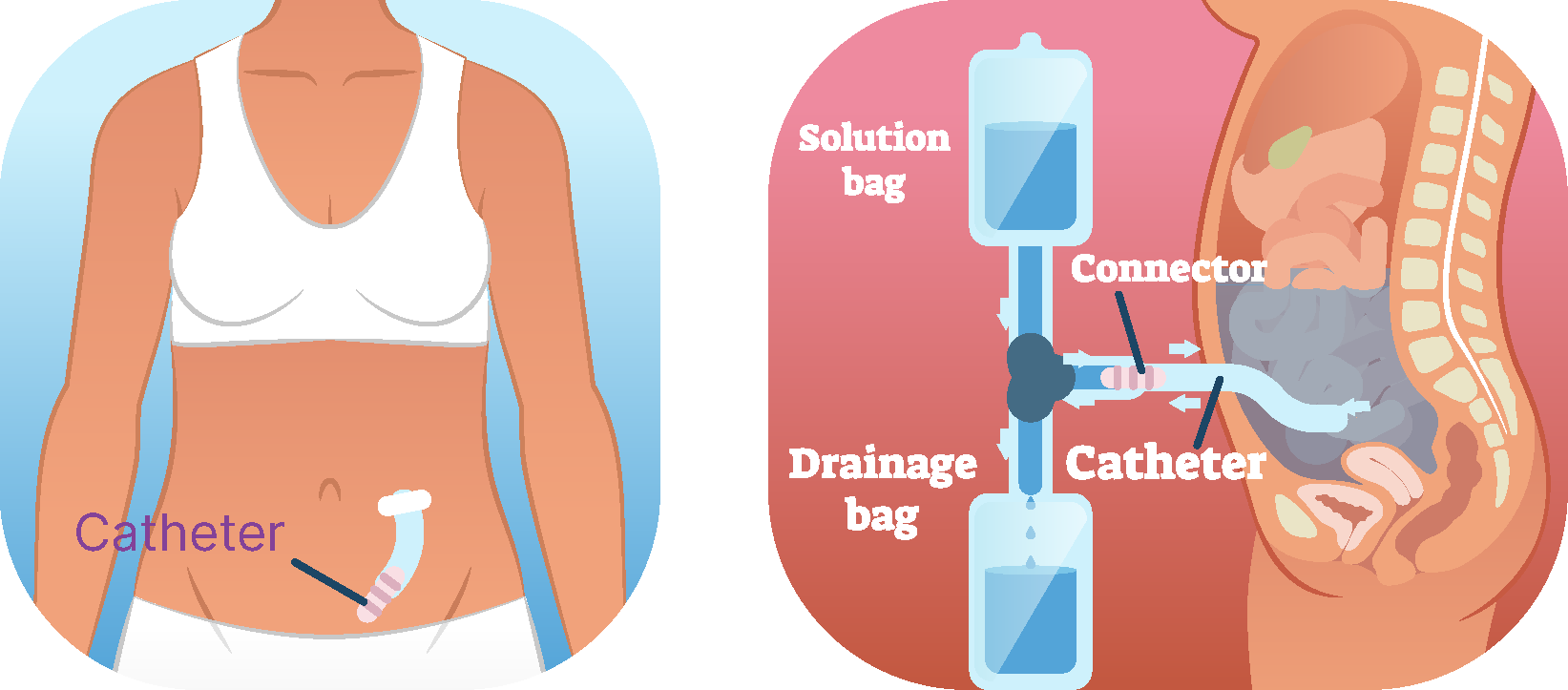
Placement of the peritoneal dialysis catheter and set up of catheter flushes until treatment begins.
The effectiveness of peritoneal dialysis as a renal replacement therapy relies on the timely establishment of a safe, functional, and long-lasting catheter access to the peritoneal cavity.1 Guidelines with regular updates ensure that practitioners remain informed of current best practice. Crabtree JH et al. Creating and maintaining optimal peritoneal dialysis access in the adult patient: 2019 update. Perit Dial Int. 2019;39(5):414-36
Educating the patient and caregiver on care and maintenance of the peritoneal dialysis catheter. Personalised patient training is key to reducing complications, enhancing patient survival, and dialysis effectiveness.1 Fernàndez Labadía E. Educational interventions and identification of risk factors to prevent and reduce peritonitis in peritoneal dialysis: a scoping review. J Ren Care. 2024;50(3):307-18
17/22
APD: automated peritoneal dialysis; CAPD: continuous ambulatory peritoneal dialysis.
The patient chooses peritoneal dialysis, which type would be the best fit?:
Continuous ambulatory peritoneal dialysis (CAPD) Standard automated peritoneal dialysis (APD) Incremental peritoneal dialysis
Answer is C CAPD is suitable for patients who prefer home-based dialysis, have preserved dexterity, and want flexibility in their schedule. However, it requires manual exchanges 3–5 times a day, which may be difficult for patients with cognitive impairment, frailty, or limited mobility.1 The patient described in this case study has cognitive impairment, therefore CAPD may not be suitable. 1. Ryan, LA. et al. Patient Outcomes of a Two-Exchange Assisted Continuous Ambulatory Peritoneal Dialysis (CAPD) Programme for Frail Older Patients: PO1265. Journal of the American Society of Nephrology 2020;31(10S):419
Answer is C APD is machine assisted overnight, reducing the need for manual exchanges. However, elderly and frail patients may require assistance to set up the machine The patient described in this case study has some remaining kidney function, is there a less intensive approach?
Answer is C Incremental peritoneal dialysis is a personalised approach that starts with lower dialysis intensity. It is beneficial for patients with some remaining kidney function that don’t yet need full dialysis support. It preserves kidney function for longer and can progress to full CAPD or APD as kidney function declines. It is suited for elderly patients where there may be a quality-of-life benefit from a reduced treatment burden. The patient is suitable for Incremental peritoneal dialysis. Brown EA. et al. International Society for Peritoneal Dialysis practice recommendations: Prescribing high-quality goal-directed peritoneal dialysis. Peritoneal Dialysis International. 2020;40(3):244-253
18/22
Include family members in the process Re-assess well-being and satisfaction with choice should be regularly assessed Incremental peritoneal dialysis
Oliver MJ et al. Assisted peritoneal dialysis: position paper for the ISPD. Perit Dial Int. 2024;44(3):160-70.
Common barriers to treatment can be overcome by the use of assisted peritoneal dialysis:1
Lack of self-care ability and family support are common barriers, but home assistance can enable these patients to receive peritoneal dialysis. Patients with cognitive decline may tolerate at home treatment better than in-centre but require assistance. Assistance increases peritoneal dialysis initiation rates and reduces transfers to haemodialysis.
Consider an a priori analysis plan to measure the cost benefits of assisted peritoneal dialysis, including indirect savings from reduced transportation, hospitalisations, nursing home admission, and avoidance of complications. Cost should account for start-up costs, skill of the assistance, number of visits provided, and duration of support.1 Oliver MJ et al. Assisted peritoneal dialysis: position paper for the ISPD. Perit Dial Int. 2024;44(3):160-70.
19/22
What is your prime goal of peritoneal dialysis for the patient?
Achieving adequacy targets Avoiding complications Meeting goals you establish with the patient Keeping dialysis volumes low to reduce burden
Answer is C The aim is to establish realistic care goals that maintain patient quality of life, minimise symptoms and treatment burden, and ensure high-quality care whilst enabling the patient to meet their life goals.1 Elderly patients constitute a diverse group of patients, and care should be individualised according to patients’ expectations and wishes:2 Standard peritoneal dialysis adequacy guidelines will be appropriate for elderly patients. Quality of life should guide care; for some, reducing treatment intensity and monitoring may be appropriate. Integrated care should prioritise end-of-life planning, but suitable patients should still have the option to switch to haemodialysis. Brown EA. International Society for Peritoneal Dialysis practice recommendations: prescribing high-quality goal-directed peritoneal dialysis. Perit Dial Int. 2020;40(3):244-53. Oei E, Fan S. Peritoneal dialysis adequacy in elderly patients. Perit Dial Int. 2015;35(6):635-9.
20/22
Take Homes
It is important to identify and discuss patient motivational factors, empowering and including patients and caregivers in decision making. Individualised dialysis modalities that maintain or improve quality of life are especially important for older patients. ‘Elderly’ patients are a diverse group with different comorbidities, life expectancies, and importantly, life expectations. Age should not be used as a criterion to deny patients home therapies; if needed, assisted peritoneal dialysis should be considered. Incremental peritoneal dialysis may benefit elderly patients by preserving residual kidney function and reducing treatment burden, improving quality-of-life.
21/22
Resources
Kidney Failure Risk Equation: https://kidneyfailurerisk.com/ KATZ Index of Independence in Activities of Daily Living (KATZ ADL): https://hign.org/sites/default/files/2020-06/Try_This_General_Assessment_2.pdf Dementia Severity Rating Scale (DSRS): https://tmdf.org/wp-content/uploads/2020/07/Dementia-Severity-Rating-Scale.pdf Multidimensional Scale of Perceived Social Support: Safi F et al. The association between self-efficacy, perceived social support, and family resilience in patients undergoing hemodialysis: a cross-sectional study. BMC Nephrol. 2024;25(1):207
22/22