Neurology
Identifying Appropriate Patients for AQUIPTA®▼ (atogepant) Through An Interactive Hypothetical Patient Case
This material is intended for healthcare professionals only. This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Treatment is always based on the needs of individual patients, and response to treatment will vary between all patients. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. This hypothetical case study is based on the EU centrally approved label for AQUIPTA®. Please refer to your local guidelines for more information. Promotional material developed and funded by AbbVie.
START
1/23
PRESCRIBING INFORMATION FOR AQUIPTA® (ATOGEPANT) AND INFORMATION ON HOW TO REPORT ADVERSE EVENTS IS AVAILABLE AT THE END OF THIS CASE STUDY
Adverse events should be reported to your local regulatory authority and AbbVie.
▼ This medicinal product is subject to additional monitoring.
ALL-AQP-250035 | March 2026
2/23
AQUIPTA® is indicated for prophylaxis of migraine in adults who have at least 4 migraine days per month1 Patient suitability for AQUIPTA® should be assessed on a case-by-case basis AbbVie does not recommend the use of products outside their licensed indications References are available upon request
Important Information
1. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025.
Claudia is a 36-year-old woman who has been experiencing migraine attacks.
Let’s meet Claudia
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available.
3/23
Migraine symptoms Claudia has two or three migraine attacks per week, with some attacks lasting up to 2 days. She believes her migraine attacks may be influenced by specific triggers:
Claudia’s current presentation
Hormonal changes
Phobias
Occupation
Health status
Recent history
Stress
Lack of sleep
Red wine consumption
Claudia has a BMI of 21 and is moderately active.
Claudia was promoted into a new, high-pressure role 6 months ago and has taken on more responsibility. Due to the nature of her work, she feels anxious about taking days off as a result of her migraine attacks.
Claudia has a phobia of needles.
Claudia is married with an 18-month-old child. She’s no longer breastfeeding and has no further pregnancies planned. She also had a copper IUD fitted for contraceptive purposes1 as she did not want to use hormonal contraception. In the last 6 months, her stress levels have increased and she’s experiencing sleep deprivation due to having a young child and the pressures of her career.
4/23
IUD: intrauterine device. 1. World Health Organization. Family planning/contraception methods. Available at: https://www.who.int/news-room/fact-sheets/detail/family-planning-contraception. Last accessed: 10 April 2025.
Claudia’s migraine attacks started at 15 years old and fluctuated in frequency during her teenage years.
Patient history
Individual product names, recommendations and indications may vary locally; please refer to your local guidance. This approach was initiated by the Danish Headache Society, and the Consensus Statement is endorsed by the European Headache Federation (EHF) and the European Academy of Neurology (EAN). The aim of the approach is to support care and clinical decision- making by primary care practitioners, neurologists and headache specialists. This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. 1. Eigenbrodt AK et al. Nat Rev Neurol. 2021;17(8):501-14.
In her 20s, her migraine frequency was 1–2 days per week.
In her 20s and 30s, Claudia self-managed her headaches.
Her migraine frequency has increased in the past 6 months.
Initially managed attacks with over-the-counter treatments (ibuprofen and paracetamol) as a teenager.1
Tried two preventive treatment options (topiramate and propranolol) in her 20s1 but discontinued treatment due to experiencing cognitive impairment and tiredness.
After discontinuing preventive treatment, she continued to use ibuprofen and paracetamol to manage her headaches.1
She has been using triptans for the past 12 months1 but experiences dizziness when taking them.
5/23
Based on Claudia’s clinical presentation and medical history, which clinical assessments would you perform? You may choose more than one option.
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. CT, computerised tomography; HIT-6: 6-item Headache Impact Test; MRI, magnetic resonance imaging.
Head CT
Blood test
Migraine days (headache diary)
HIT-6
A
B
C
D
Migraine triggers (headache diary)
E
Head MRI
F
SUBMIT
6/23
Here is what Claudia's doctor chose.
HIT-6: To determine the impact of migraine on Claudia’s quality of life,1 including:2
Rationale for choosing these clinical assessments
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. HIT-6: 6-item Headache Impact Test.
Frequency of headaches with severe pain Impact of headache on daily activities Impact of headache on functionality
Impact of headache on energy Impact of headache on mood Impact of headache on concentration
Headache diary:3 To track the number of migraine days and determine any of the potential triggers or patterns of migraine that Claudia has identified.
References
HIT-6: Results of clinical assessments Patient score Score: 581
Headache diary:3 Results of clinical assessments Patient diary report Reported migraine attacks on an average of 8 days per month. Reported headaches on an average of 3 days per month. Approximately 75% of her migraine attacks were strongly linked to a reported feeling of stress and/or lack of sleep.
Headache diary:3 Results of clinical assessments Patient diary report Claudia felt there was a mild link between migraine onset and drinking red wine. There was no strong link between migraine attacks and hormonal changes.
1. Yang M et al. Cephalalgia. 2011;31(3):357-67. 2. Migraine Canada. HIT-6™. Available at: https://migrainecanada.org/wp-content/uploads/2020/02/HIT-6-test-english.pdf. (Accessed: 8 May 2025) 3. The Migraine Trust. Keeping a headache diary. Available at: https://migrainetrust.org/live-with-migraine/self-management/keeping-a-migraine-diary/ (Accessed: 8 May 2025).
7/23
What is the significance of a HIT-6 score of 58? You may choose one option.
Little or no impact
Some impact
Substantial impact
Severe impact
HIT-6 grading1 Scores ≤49: Little or no impact Scores 50–55: Some impact Scores 56–59: Substantial impact Scores 60–78: Severe impact 1. Yang M et al. Cephalalgia. 2011;31(3):357-67.
8/23
Which diagnoses do not apply to Claudia based on the information presented? You may choose more than one option.
Chronic tension-type headache
Episodic migraine
Chronic migraine
Migraine without aura
Cluster headache
Migraine with aura
9/23
Migraine without aura*1 Claudia’s attacks aligned with the symptoms and duration of migraine attacks. She did not experience any additional aura symptoms.
Claudia fulfilled the criteria for migraine without aura and episodic migraine
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. *Please refer to the ICHD-3 for the full diagnostic criteria for migraine with aura.1 ICHD-3: International Classification of Headache Disorders, 3rd edition.
The rationale for this diagnosis is below.
Episodic migraine1 Claudia experienced migraine attacks within the 4–14-day range.
1. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211.
10/23
Patient treatment options
Following Claudia’s assessment, several treatment options were considered.
This is a hypothetical patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. CGRP: calcitonin gene-related peptide; mAb: monoclonal antibody. 1. Eigenbrodt AK et al. Nat Rev Neurol. 2021;17(8):501-14.
Which treatment would you consider for Claudia? You may choose one option.
Following Claudia’s assessment, several management options were considered.
Gepants
CGRP mAbs1
Topiramate1
Other
Chosen preventive treatment: AQUIPTA® (atogepant) 60 mg oral tablet, taken once daily2
Which additional management would you consider appropriate for Claudia? You may choose one option.
Counselling
Stress management (e.g. meditation)
Diet and exercise
11/23
2. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025.
Rationale for preventive treatment
Following diagnosis, Claudia discussed her preferences for treatment moving forward.
Claudia outlined the following considerations:
Claudia’s concerns around using preventive treatment were discussed:
Acute vs preventive Preference for acute treatment due to bad experience with previous preventive treatments, but willing to discuss current preventive options that are available. Aspires to manage her migraine attacks.
Treatment administration Preference for oral treatments over subcutaneous injections due to phobia of needles.
She was educated on the current preventive treatment landscape, including the tolerability profiles of different treatment options. Due to the severity of her migraine attacks and the information she had been given, she agreed to try a preventive treatment.
12/23
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. 1. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025; 2. Eigenbrodt AK et al. Nat Rev Neurol. 2021;17(8):501-14.
What information is important to discuss with Claudia before initiating treatment with AQUIPTA®? You may choose more than one option.
Ensuring AQUIPTA® is taken once daily1
Education on the differences between acute and preventive treatment1,2
Education around potential side effects1
13/23
Let’s hear from Claudia about her treatment plan
14/23
A treatment follow-up was arranged 3 months after treatment initiation. What treatment outcomes would you expect to see for Claudia? You may choose more than one option.
Reduction in monthly migraine days
Reduction in stress levels (patient reported)
Improvement in amount of sleep per night (patient reported)
Reduction in acute medication use
15/23
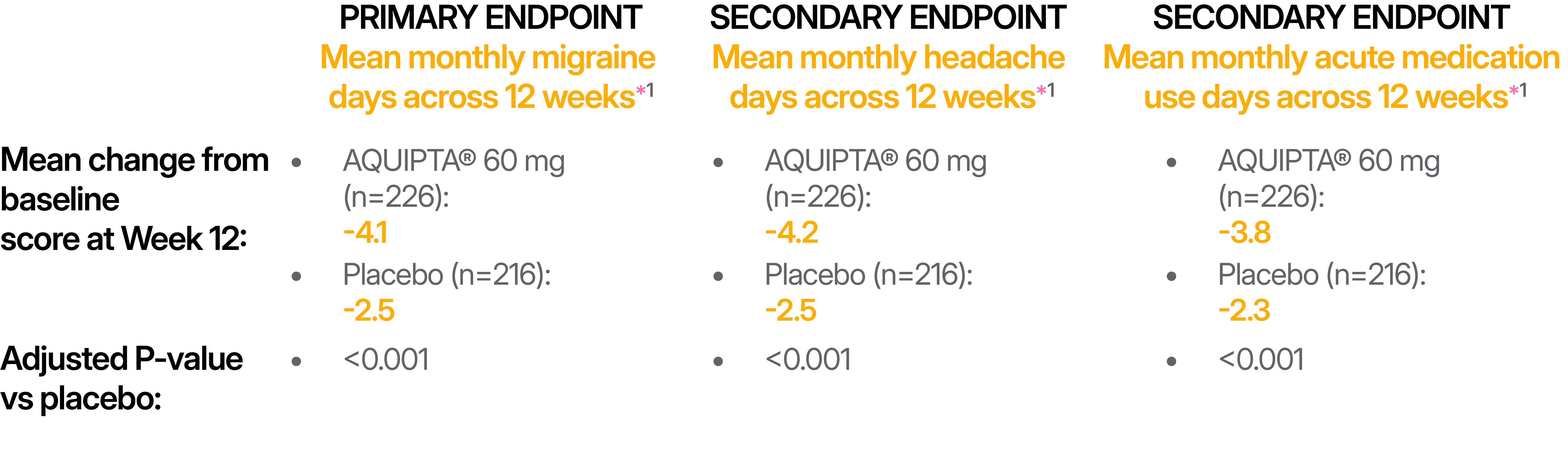
ADVANCE trial in episodic migraine: Primary and secondary endpoints in AQUIPTA® vs placebo.*1
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. *Participants were included in the off-treatment hypothetical estimated population. †This study was a secondary analysis of the ADVANCE study and was carried out to evaluate the efficacy and safety of AQUIPTA® for the preventive treatment of migraine (4–14 migraine days per month).1
At Week 12, there was a significant difference in the response rate for the reduction in mean month migraine days within the double-blind treatment period with AQUIPTA® 60 mg vs placebo.†2 59.0% of patients achieved a ≥50% reduction in mean monthly migraine days with AQUIPTA® vs 29.0% with placebo across 12 weeks (P<0.001).1 Predefined secondary endpoint.*1 Several patient-reported outcomes measures assessing functioning were assessed during the ADVANCE trial, with significant results reported vs placebo.1
1. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/-documents/product-informa-tion/aquipta-epar-product-informat-ion_en.pdf. Last accessed: 13 August 2025; 2. Lipton RB, et al. JAMA Netw Open. 2022;5(6):e2215499.
16/23
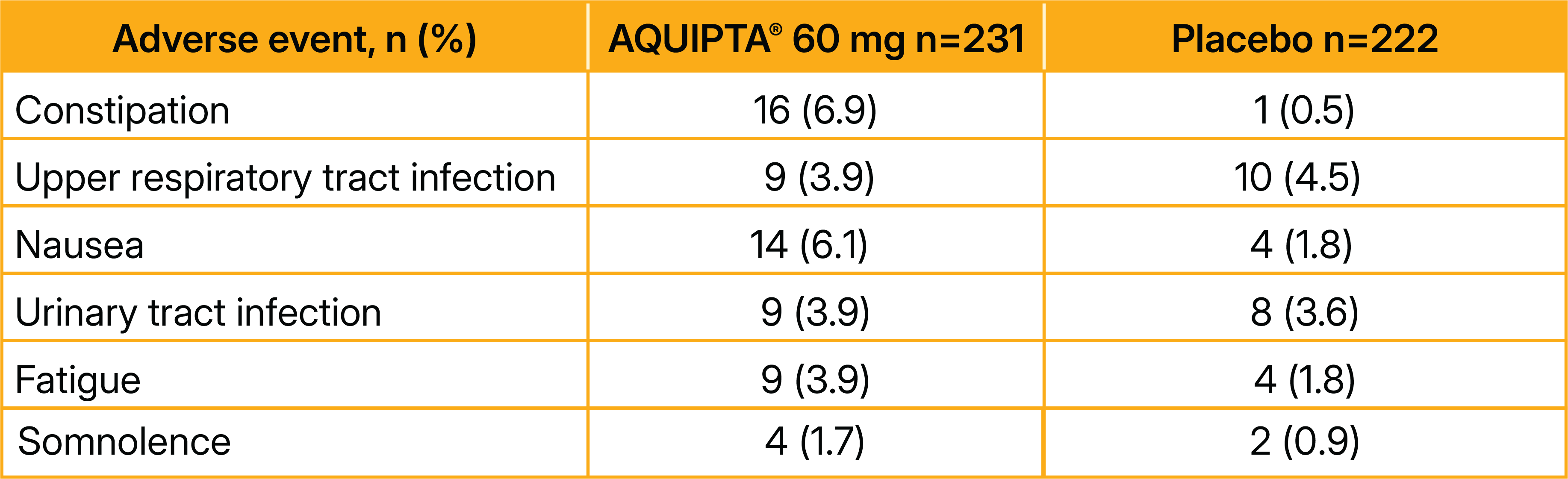
Adverse events were recorded if they began or worsened on or after the date of the first dose of AQUIPTA® or placebo until 30 days after the last dose1 The most common adverse events reported in ≥2% of participants in the AQUIPTA® 60 mg group were:1
The ADVANCE trial in episodic migraine: Adverse events reported*1
*Efficacy and safety of the AQUIPTA® 10 mg dose were also assessed within the ADVANCE trial.1 Efficacy and safety of the AQUIPTA® 10 mg dose were similar to those of the 60 mg dose.1 The AQUIPTA® 10 mg dose is recommended for dose modification and special populations.2 For further information, please refer to your local licence and guidelines.2 †The safety population results were based on the modified intent-to-treat population.1 ‡The relatedness of adverse events to AQUIPTA® or placebo was determined by the investigator.1 1. Ailani J et al. N Engl J Med. 2021;385(8):695-706; 2. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025.
The frequency of adverse events reported was 53.7% in the AQUIPTA® 60 mg group (n=231), compared with 56.8% in the placebo group (n=222)†1
Table adapted from Ailani J, et al. 2021.1
17/23
A similar efficacy and safety profile was reported for the AQUIPTA® 10 mg dose throughout the ADVANCE study*,†,1
Table adapted from Ailani J et al. 2021.1
AQUIPTA® is not recommended during pregnancy or in women of childbearing potential not using contraception.1 The developmental and health benefits of breast-feeding should be considered along with the mother’s clinical need for AQUIPTA® and any potential adverse effects on the breastfed infant from AQUIPTA® or from the underlying maternal condition.1 AQUIPTA® is not recommended in patients with severe hepatic impairment.1 The most commonly reported adverse drug reactions are nausea, constipation and fatigue/somnolence.1 Serious hypersensitivity reactions, decreased appetite, weight decreased and increased ALT/AST have been reported.1
AQUIPTA® safety information
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Other treatment options are available. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. ALT: alanine aminotransferase; AST: aspartate aminotransferase. 1. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025.
18/23
Case summary
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Other treatment options for migraine are available. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. 1. AbbVie Deutschland GmbH & Co. KG Ludwigshafen Germany. AQUIPTATM (atogepant) Summary of Product Characteristics. 2025. Available at: https://www.ema.europa.eu/en/documents/product-information/aquipta-epar-product-information_en.pdf. Last accessed: 13 August 2025; 2. Ailani J et al. N Engl J Med. 2021;385(8):695–706.
Claudia had experienced migraine attacks since she was a teenager; they had increased in severity over the past 6 months.
After discussions with her doctor, Claudia hoped that her treatment plan would reduce the frequency of her migraine attacks.
Results from the Phase III, double-blind, placebo-controlled ADVANCE trial showed that once-daily AQUIPTA® 60 mg showed significant improvement in migraine symptoms, headache symptoms and patient-reported outcomes vs placebo.1,2
19/23
Mandatory Information Norway Product name: Aquipta (atogepant) tablets Indication: AQUIPTA is indicated for prophylaxis of migraine in adults who have at least 4 migraine days per month. Selected Safety Information Not recommended during pregnancy and in women of childbearing potential not using contraception. The choice between breastfeeding or treatment must be assessed on the basis of benefit/risk. Not recommended in patients with severe hepatic impairment. The most commonly reported adverse drug reactions are nausea, constipation, and fatigue/somnolence. Serious hypersensitivity reactions, decreased appetite, weight decreased, and increased ALAT/AST have been reported. Dosage: The recommended dose is 60 mg once daily. With the use of strong CYP3A4 inhibitors or strong OATP inhibitors, in severe renal impairment or end-stage renal disease, the recommended dose is 10 mg once daily. Swallowed whole. Packaging and prices: 10 mg: 28 tabl.: kr 3 931,70. 60 mg: 28 tabl.: kr 3931.70 Aquipta har ikke forhåndsgodkjent refusjon. Individuell stønad kan søkes ved forebyggende behandling av kronisk migrene iht. de vilkår/krav som er angitt i vedlegg 1 til Folketrygdloven § 5-14 (legemiddellisten). Prescription group: C. For mer informasjon om dosering, kontraindikasjoner, forsiktighetsregler og bivirkninger, se Aquipta SPC 08.05.2025
For Norwegian HCPs only
This is a hypothetical AQUIPTA®-treated patient case study developed in collaboration with an expert based on their experience. Case studies are intended to encourage scientific debate and exchange, and to enhance appropriate patient management. Case studies are representative only, and individual patient responses may vary. Other treatment options are available. Clinical assessments and treatment options discussed in this case are not an exhaustive list of options available. CYP, cytochrome; HCP, healthcare professional; OATP, Organic Anion Transporting Polypeptide.
20/23
Prescribing information - Sweden AQUIPTA® (atogepant). Analgesics, calcitonin gene-related peptide (CGRP) antagonists (ATC code: N02CD07), tablet 10 mg, 60 mg (Rx, (F)). Swallowed whole. Indication: prophylaxis of migraine in adults who have at least 4 migraine days per month. Contraindications: hypersensitivity to the active substance or to any of the excipients. Warnings and precautions: concomitant use of strong CYP3A4 inhibitors and OATP inhibitors, use in patients with severe renal impairment and end-stage renal disease, the recommended dose is 10 mg once daily. Should be avoided in patients with severe hepatic impairment. Serious hypersensitivity reactions have been reported. Fertility, pregnancy and lactation: not recommended during pregnancy and in women of childbearing potential not using contraception. Pharmacokinetic data after single-dose administration showed minimal transfer of atogepant into breast milk. There are no data on the effects of atogepant on the breastfed infant or on milk production. Treatment during breast-feeding should be considered along with the mothers clinical need for atogepant. Restriction of reimbursement: AQUIPTA is reimbursed only for patients with chronic migraine who, after optimized treatment, have not had effect of or have not tolerated at least two different prophylactic drug therapies. Reimbursed only when prescribed by neurologist or physician operating at a neurology clinic or clinic/unit specialized in the treatment of patients with chronic migraine. For further information about the product and latest price information see www.fass.se. Date of revision of the Summary of Product Characteristics: 2025-05-08. AbbVie AB, +46 (0)8 684 44 600, info@abbvie.se. ▼ This medicinal product is subject to additional monitoring.
21/23
Prescribing information (Sweden)
Please click the relevant country: Finland Germany Spain Portugal Norway Sweden
Prescribing information
22/23
THANK YOU
23/23